Benchmarking in Healthcare: Industrial Engineering and ISE Perspectives
Benchmark is one of important aspects in Industrial Engineering (IE), including within Industrial and Systems Engineering Perspectives. Product Design Engineering (PDE) program in Binus Aso School of Engineering (BASE) ensures that PDE students in BASE intertwine the competencies of both IE and PDE. The reason behind that intertwined IE and PDE are to maintain the benchmark within the most sustain and improvement of Plan Do Check Act (PDCA) cycle, toward Competitive Advantages.
Source: ISE Magazine 2019 (Industrial and Systems Engineering (ISE) 2019)
Author: Peter Woodbridge
Recently, a young engineering colleague in the steel industry described his benchmarking visit to another facility. While observing differences in process, he was frustrated that engineers at the other facility could not explain why they selected specific parameters and procedures. He wondered if the differences were strictly contextual or pointed to better processes he might bring back to his own facility after validation.
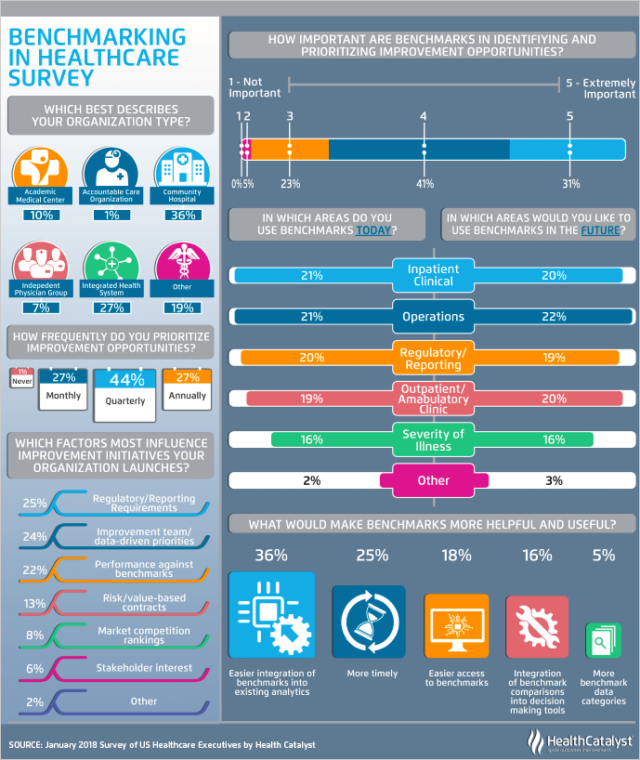
Benchmarking is used extensively in healthcare – or widely “misused” in healthcare. Underperforming entities in health system organizations are encouraged to learn from those performing better. The benchmarking visits end up being as unsatisfying as that of the young engineer. Staff members at the better performing facility cannot explain why they do what they do. Staff from the underperforming facility either dismisses the other site’s success as contextual or commits to change without understanding. Unlike the young engineer, they rarely have the knowledge, support or resources to conduct their own validation studies.
There are exceptions.
Kaiser Permanente used benchmarking to successfully optimize its performance improvement system (“Kaiser Permanente’s Performance Improvement System, Part 1: From Benchmarking to Executing on Strategic Priorities,” 2010). Kaiser Permanente is one of the largest health system organizations in the U.S and serves 12.3 million members. Through judicious benchmarking inquiry and analysis, it identified the essential features for systemwide performance improvement. In a novel approach, Intermountain Healthcare (IHC) uses a twist on benchmarking to improve quality and patient safety by reducing interprovider variation.
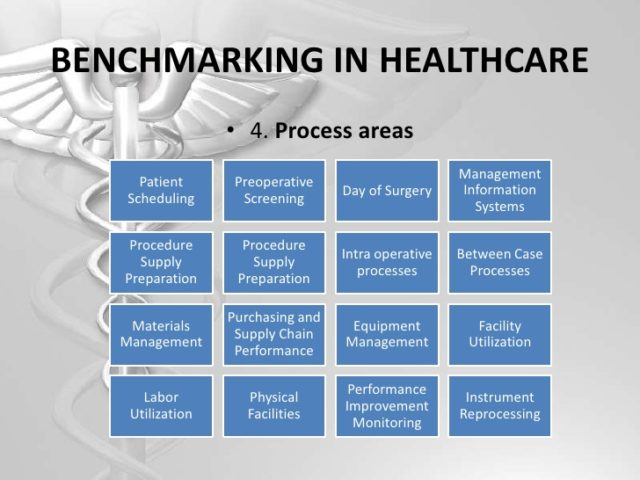
IHC begins by identifying high priority clinical processes (National Academy Press, 2011). High priority clinical processes carry high risk to individual patients and affect high volumes of patients. IHC then convenes teams with representatives of all services that impact the process. The team is not limited to clinical staff and includes administrative staff for supporting functions. The team maps the process, analyzes variation and identifies key measures of quality, utilization and efficiency. Since data in healthcare information systems is generally not reflective of clinical workflows and processes, IHC developed specialized systems for data gathering and analysis. Based on this, teams develop evidence-based best practice guidelines blended into clinical workflow, training, logistics and measurement and analysis. That becomes a shared baseline used as a benchmark against which individual and system performance is measured. Shared baselines differ from most evidence-based guidelines, as rigid adherence is not expected and, in fact, is discouraged. Physicians and other clinical providers are expected to adapt shared baselines for patient individuality.

From the Roundtable: “A physician will undergo just as much scrutiny for complying with a shared baseline too often, as compared to his or her peers, as for complying too infrequently.” Deviations are either opportunities for improving the shared baseline or for individual provider learning. When a new baseline is implemented, it typically undergoes hundreds of modifications in its first year to support organizational learning and address provider antipathy to cookbook medicine. In industry, benchmarking is used to focus continuous improvement. In many instances, the experience does not live up to its potential when sites being benchmarked do not have a full understanding of factors that contribute to higher performance. The same is true in healthcare, where processes and factors critical to success, while perhaps evidence-based through research, are not well integrated into workflow. Kaiser Permanente and IHC are exceptions where benchmarking has been successfully used to improve quality and reduce patient harm.
Comments :